
Medullary osmotic gradient: countercurrent multiplier, urea recycling & vasa recta countercurrent exchange

By: HWC
Date Uploaded: 11/06/2019
Tags: homeworkclinic.com Homework Clinic HWC Medullary osmotic gradient countercurrent multiplier medullary osmotic gradient osmolarity Squamous epithelial cells cuboidal epithelial cells Henle medullar space nephron tubules vasa recta countercurrent exchange Blood osmolarity nephron
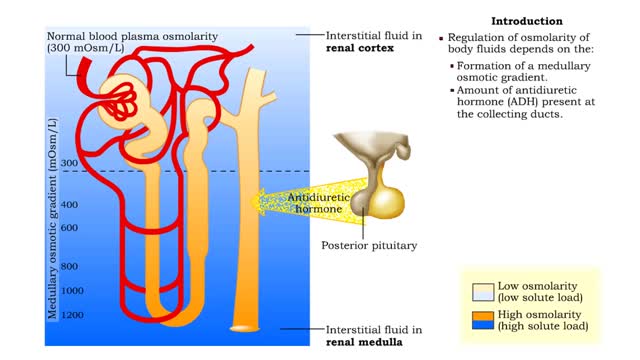
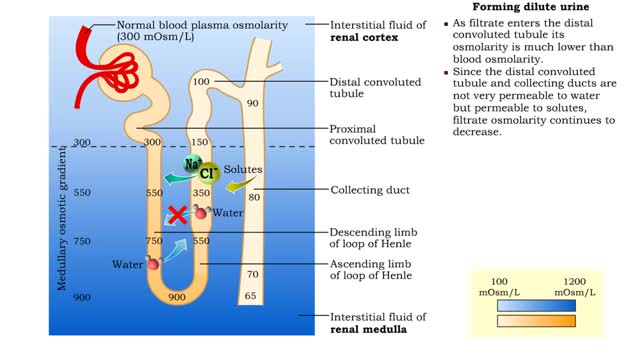
▪ The primary cause of the medullary osmotic gradient is the active transport of solutes. • In the ascending limb of the loop, active transport of Na+ ions drives passive reabsorption of Cl- ions. • Addition of these ions to the interstitial fluid of the medulla increases its osmolarity. • Squamous epithelial cells of the descending limb of the loop are permeable to water but impermeable to most solutes. • Water leaves the filtrate in the descending limb of the loop, but the solutes cannot enter, thus increasing the filtrate osmolarity. • Due to water movement, new filtrate entering the descending limb becomes more and more concentrated as it flows to the bottom of the loop. • The cuboidal epithelial cells of the ascending limb provide for active reabsorption of Na+ and Cl- ions, but are impermeable to water. • Due to active reabsorption of solutes along the ascending limb, the filtrate being concentrated in the loop bottom becomes more and more diluted towards the distal convoluted tubule. • The limbs of the loop are close enough that each influences the processes occurring in the other. • Water moves out of the descending limb and produces the more "salty" filtrate toward the loop bottom. • In the ascending limb, the solutes pumped out of the concentrated filtrate increase the medullary osmotic gradient. • More solutes leaving the ascending limb cause more water to leave the descending limb and vice versa. • These processes multiply each other until the dynamic equilibrium is achieved between osmolarity of fluids in the different limbs of the loop of Henle and the surrounding medullar space. • This mechanism that constantly establishes the osmolarity gradient thoughout the renal medulla is called the countercurrent multiplier. • The effect of urea recycling greatly increases the medullary osmotic gradient values to their final amounts. ▪ When filtrate enters the medullary part of the collecting duct, most water has been reabsorbed, leaving urea relatively concentrated. • Collecting duct cells are highly permeable to urea, so urea diffuses into the medulla, thus increasing the interstitial osmolarity. • The rest of the nephron tubules are poorly permeable to urea, therefore, the urea is recycled back to the collecting duct in the medulla. • Along with sodium chloride, urea provides a great deal of the solute load in the medulla, producing much of the medullary osmotic gradient. • An ordinary capillary carrying blood from the cortex, and through the medulla, would remove the solutes necessary to generate the medullary osmotic gradient. • The shape of the vasa recta follows the limbs of the loop, providing a mechanism to maintain the gradient. • Blood enters the medulla of the kidney with normal osmolarity. • As blood moves into the medulla, highly permeable vasa recta capillaries exchange solutes with interstitial fluid. • Blood osmolarity increases. • As the blood moves out of the medulla, up to the cortex, it loses solutes. • Blood osmolarity decreases nearly to the normal value. • The small increase of osmolarity in the blood leaving the vasa recta: • Is the result of the blood colloid osmolarity. • Indicates that some water is lost from the body. • Tissues are provided with nutrients and oxygen, but solutes that maintain the medullary osmotic gradient are not transported away from the nephron.
Add To
You must login to add videos to your playlists.
Advertisement
Suggestions

Comments
0 Comments total
Sign In to post comments.
No comments have been posted for this video yet.